
AmBetter from Buckeye Health Plan
Plan Overviews
Ambetter from Superior HealthPlan provides quality healthcare solutions that help residents of Ohio live better. With a variety of affordable coverage options, they make it easier to stay healthy.
Ambetter health insurance plans offer 2 levels of plan options (Silver and Gold – Ambetter does not currently offer Bronze plans), each one representing a different type of coverage and payment. However, no matter which Ambetter plan you choose, you can always count on access to high quality, comprehensive care that delivers services, support and all of your Essential Health Benefits.
Apply Online Now

Plan Name |
Balanced Care 1 |
Balanced Care 2 |
Balanced Care 10 |
Balanced Care 12 |
| Medical Deductible (Ind/Fam) | $5,500/$11,000 | $6,500/$13,000 | $4,500/$9,000 | $3,500/$7,000 |
| Prescription Drug Deductible (Ind/Fam) | Integrated with medical ded. | Integrated with medical ded. | Integrated with medical ded. | Integrated with medical ded. |
| Out-of-pocket Maximum (Ind/Fam) | $6,500/$13,000 | $6,500/$13,000 | $6,500/$13,000 | $7,150/$14,300 |
| Annual Well Visit/ Preventive Care | No charge | No charge | No charge | No charge |
| PCP Office Visit | 30 | 30 | 20 | 30 |
| Specialist Office Visit | 60 | 60 | 40 | 65 |
| Imaging(CT/PET Scans, MRIs) | 20% after ded. | No charge after ded. | 20% after ded. | 20% after ded. |
| X-rays & Diagnostic Imaging | 20% after ded. | No charge after ded. | 20% after ded. | 20% after ded. |
| Urgent Care | 100 | 100 | 100 | 75 |
| Emergency Room* | 20% after ded. | No charge after ded. | 20% after ded. | $400 after ded. |
| Emergency Transportation* | 20% after ded. | No charge after ded. | 20% after ded. | 20% after ded. |
| Inpatient Facility Fee | 20% after ded. | No charge after ded. | 20% after ded. | 20% after ded. |
| Inpatient Hospital Physician & Surgical Services | 20% after ded. | No charge after ded. | 20% after ded. | 20% after ded. |
| Outpatient Facility Fee | 20% after ded. | No charge after ded. | 20% after ded. | 20% after ded. |
| Outpatient Surgery Physician/Surgical Services | 20% after ded. | No charge after ded. | 20% after ded. | 20% after ded. |
| Labs & Diagnostics | 20% after ded. | No charge after ded. | 20% after ded. | 20% after ded. |
| Mental/Behavioral Health & Substance Use Disorder Outpatient Services | 30 | 30 | 20 | 30 |
| Rehabilitation Outpatient Services (Includes Speech, Occupational, Physical Therapy) | 20% after ded. | No charge after ded. | 20% after ded. | 20% after ded. |
| Skilled Nursing Facility | 20% after ded. | No charge after ded. | 20% after ded. | 20% after ded. |
| Pediatric Vision- Routine Eye Exam (1 visit per year) | 100% Covered | 100% Covered | 100% Covered | 100% Covered |
| PediatricVision- Eyeglasses (frames, 1 per year) | 100% Covered | 100% Covered | 100% Covered | 100% Covered |
| PedicatricVision- Lenses (per pair) | 100% Covered | 100% Covered | 100% Covered | 100% Covered |
| Pharmacy* (Generic / Preferred / Non-preferred / Specialty) |
$10 / $50 / 20% after Rx ded. / 20% after Rx ded. | $15 / $50 / No charge after ded. / No charge after ded. | $10 / $50 / 20% after ded. / 20% after ded. | $15 / $50 / $100 / 40% |
Plan Name |
Secure Care 1 (2017) with 3 Free PCP Visits |
| MedicalDeductible (Ind/Fam) | $1,000/$2,000 |
| PrescriptionDrug Deductible (Ind/Fam) | $500/$1,000 |
| Out-of-pocketMaximum (Ind/Fam) | $6,350/$12,700 |
| Annual Well Visit/ Preventive Care | No charge |
| PCP Office Visit | 20% after ded. |
| Specialist Office Visit | 20% after ded. |
| Imaging(CT/PET Scans, MRIs) | 20% after ded. |
| X-rays & Diagnostic Imaging | 20% after ded. |
| Urgent Care | 20% after ded. |
| Emergency Room | $250 after ded. |
| Emergency Transportation | 20% after ded. |
| Inpatient Facility Fee | 20% after ded. |
| Inpatient Hospital Physician & Surgical Services | 20% after ded. |
| Outpatient Facility Fee | 20% after ded. |
| Outpatient Surgery Physician/Surgical Services | 20% after ded. |
| Labs & Diagnostics | 20% after ded. |
| Mental/Behavioral Health & Substance Use Disorder Outpatient Services | 20% after ded. |
| RehabilitationOutpatient Services (Includes Speech, Occupational, Physical Therapy) | 20% after ded. |
| Skilled Nursing Facility | 20% after ded. |
| PediatricVision- Routine Eye Exam (1 visit per year) | 100% Covered |
| PediatricVision- Eyeglasses (frames, 1 per year) | 100% Covered |
| PedicatricVision- Lenses (per pair) | 100% Covered |
| Pharmacy (Generic / Preferred / Non-preferred / Specialty) |
$10 / $25 after Rx ded. / $75 after Rx ded. / 30% after Rx ded. |
Ambetter Health Insurance Plans Offer:
![]()
Comprehensive Medical Coverage
Complete medical coverage that meets your medical needs and contains all of the Essential Health Benefits.
![]()
24/7 Nurse Advice Line
Call and talk to a medical professional about your immediate health needs—at any time.
![]()
My Health Pays™ Rewards Program
Earn reward dollars just by staying proactive about your health.
![]()
Prescription Coverage
Get coverage for your medical prescriptions.
![]()
Integrated Care Management
Get well and stay well with preventive care and whole health services.
![]()
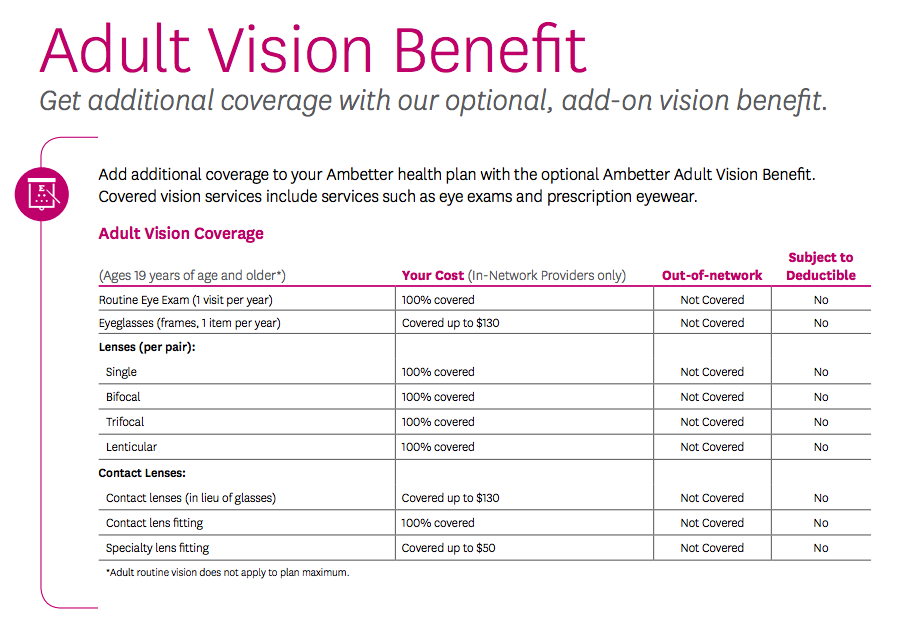
Optional Adult Vision Coverage*
Coverage for services such as eye exams and prescription eyewear.
Apply Online Now
Ambetter Ohio Coverage Map
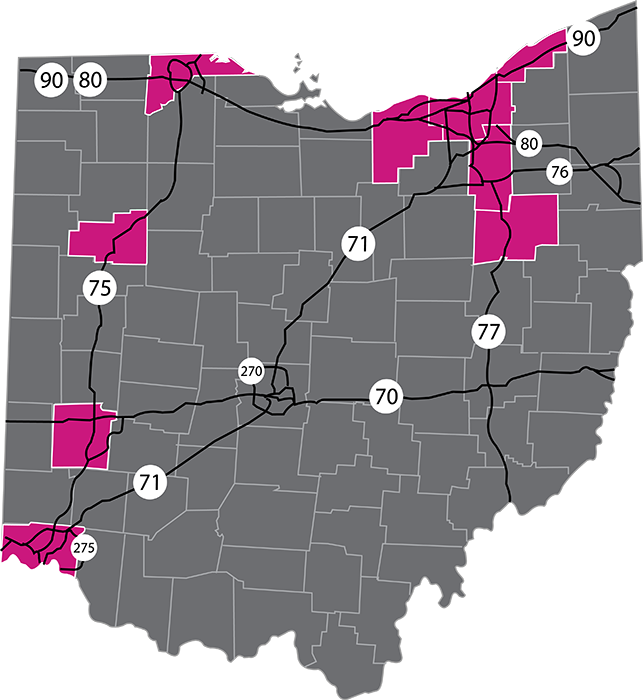
Coverage is available in:
Allen
Cuyahoga
Hamilton
Lake Lorain
Lucas
Montgomery
Stark
Summit
Plan Brochures
Plan Name |
Federal Poverty Level |
Deductible |
Out-Of-Pocket |
Coinsurance |
Brochures |
Summary of Benefits |
| Ambetter Balanced Care 10 (2017) + Vision + Adult Dental (94% AV Cost Share) | 100%-150% | $250 | $550 | 20% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 10 (2017) + Vision + Adult Dental (87% AV Cost Share) | 150%-200% | $1,000 | $1,750 | 20% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 10 (2017) + Vision + Adult Dental (73% AV Cost Share) | 200%-250% | $4,000 | $5,500 | 20% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 10 (2017) + Vision + Adult Dental (Limited Cost Share) | 300% and Above, AIAN* | $4,500 | $6,500 | 20% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 10 (2017) + Vision + Adult Dental (Zero Cost Share) | 300% and Below, AIAN* | $0 | $0 | 0% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 10 (2017) + Vision + Adult Dental (Standard Cost Share) | 250% and Above | $4,500 | $6,500 | 20% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 10 (2017) + Vision + Adult Dental (Standard Cost Share) | 250% and Above | $4,500 | $6,500 | 20% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 2 (2017) + Vision + Adult Dental (94% AV Cost Share) | 100%-150% | $575 | $575 | 0% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 2 (2017) + Vision + Adult Dental (87% AV Cost Share) | 150%-200% | $1,750 | $1,750 | 0% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 2 (2017) + Vision + Adult Dental (73% AV Cost Share) | 200%-250% | $5,000 | $5,000 | 0% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 2 (2017) + Vision + Adult Dental (Limited Cost Share) | 300% and Above, AIAN* | $6,500 | $6,500 | 0% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 2 (2017) + Vision + Adult Dental (Zero Cost Share) | 300% and Below, AIAN* | $0 | $0 | 0% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 2 (2017) + Vision + Adult Dental (Standard Cost Share) | 250% and Above | $6,500 | $6,500 | 0% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 2 (2017) + Vision + Adult Dental (Standard Cost Share) | 250% and Above | $6,500 | $6,500 | 0% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 1 (2017) + Vision + Adult Dental (94% AV Cost Share) | 100%-150% | $0 | $700 | 20% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 1 (2017) + Vision + Adult Dental (87% AV Cost Share) | 150%-200% | $450 | $2,250 | 20% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 1 (2017) + Vision + Adult Dental (73% AV Cost Share) | 200%-250% | $3,500 | $5,450 | 20% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 1 (2017) + Vision + Adult Dental (Limited Cost Share) | 300% and Above, AIAN* | $5,500 | $6,500 | 20% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 1 (2017) + Vision + Adult Dental (Zero Cost Share) | 300% and Below, AIAN* | $0 | $0 | 0% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 1 (2017) + Vision + Adult Dental (Standard Cost Share) | 250% and Above | $5,500 | $6,500 | 20% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 1 (2017) + Vision + Adult Dental (Standard Cost Share) | 250% and Above | $5,500 | $6,500 | 20% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 10 (2017) + Vision (94% AV Cost Share) | 100%-150% | $250 | $550 | 20% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 10 (2017) + Vision (87% AV Cost Share) | 150%-200% | $1,000 | $1,750 | 20% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 10 (2017) + Vision (73% AV Cost Share) | 200%-250% | $4,000 | $5,500 | 20% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 10 (2017) + Vision (Limited Cost Share) | 300% and Above, AIAN* | $4,500 | $6,500 | 20% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 10 (2017) + Vision (Zero Cost Share) | 300% and Below, AIAN* | $0 | $0 | 0% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 10 (2017) + Vision (Standard Cost Share) | 250% and Above | $4,500 | $6,500 | 20% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 10 (2017) + Vision (Standard Cost Share) | 250% and Above | $4,500 | $6,500 | 20% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 2 (2017) + Vision (94% AV Cost Share) | 100%-150% | $575 | $575 | 0% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 2 (2017) + Vision (87% AV Cost Share) | 150%-200% | $1,750 | $1,750 | 0% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 2 (2017) + Vision (73% AV Cost Share) | 200%-250% | $5,000 | $5,000 | 0% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 2 (2017) + Vision (Limited Cost Share) | 300% and Above, AIAN* | $6,500 | $6,500 | 0% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 2 (2017) + Vision (Zero Cost Share) | 300% and Below, AIAN* | $0 | $0 | 0% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 2 (2017) + Vision (Standard Cost Share) | 250% and Above | $6,500 | $6,500 | 0% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 2 (2017) + Vision (Standard Cost Share) | 250% and Above | $6,500 | $6,500 | 0% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 1 (2017) + Vision (94% AV Cost Share) | 100%-150% | $0 | $700 | 20% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 1 (2017) + Vision (87% AV Cost Share) | 150%-200% | $450 | $2,250 | 20% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 1 (2017) + Vision (73% AV Cost Share) | 200%-250% | $3,500 | $5,450 | 20% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 1 (2017) + Vision (Limited Cost Share) | 300% and Above, AIAN* | $5,500 | $6,500 | 20% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 1 (2017) + Vision (Zero Cost Share) | 300% and Below, AIAN* | $0 | $0 | 0% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 1 (2017) + Vision (Standard Cost Share) | 250% and Above | $5,500 | $6,500 | 20% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 1 (2017) + Vision (Standard Cost Share) | 250% and Above | $5,500 | $6,500 | 20% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 12 (2017) (94% AV Cost Share) | 100%-150% | $250 | $1,250 | 5% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 12 (2017) (87% AV Cost Share) | 150%-200% | $700 | $2,000 | 20% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 12 (2017) (73% AV Cost Share) | 200%-250% | $3,000 | $5,700 | 20% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 12 (2017) (Limited Cost Share) | 300% and Above, AIAN* | $3,500 | $7,150 | 20% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 12 (2017) (Zero Cost Share) | 300% and Below, AIAN* | $0 | $0 | 0% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 12 (2017) (Standard Cost Share) | 250% and Above | $3,500 | $7,150 | 20% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 12 (2017) (Standard Cost Share) | 250% and Above | $3,500 | $7,150 | 20% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 10 (2017) (94% AV Cost Share) | 100%-150% | $250 | $550 | 20% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 10 (2017) (87% AV Cost Share) | 150%-200% | $1,000 | $1,750 | 20% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 10 (2017) (73% AV Cost Share) | 200%-250% | $4,000 | $5,500 | 20% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 10 (2017) (Limited Cost Share) | 300% and Above, AIAN* | $4,500 | $6,500 | 20% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 10 (2017) (Zero Cost Share) | 300% and Below, AIAN* | $0 | $0 | 0% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 10 (2017) (Standard Cost Share) | 250% and Above | $4,500 | $6,500 | 20% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 10 (2017) (Standard Cost Share) | 250% and Above | $4,500 | $6,500 | 20% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 2 (2017) (94% AV Cost Share) | 100%-150% | $575 | $575 | 0% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 2 (2017) (87% AV Cost Share) | 150%-200% | $1,750 | $1,750 | 0% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 2 (2017) (73% AV Cost Share) | 200%-250% | $5,000 | $5,000 | 0% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 2 (2017) (Limited Cost Share) | 300% and Above, AIAN* | $6,500 | $6,500 | 0% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 2 (2017) (Zero Cost Share) | 300% and Below, AIAN* | $0 | $0 | 0% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 2 (2017) (Standard Cost Share) | 250% and Above | $6,500 | $6,500 | 0% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 2 (2017) (Standard Cost Share) | 250% and Above | $6,500 | $6,500 | 0% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 1 (2017) (94% AV Cost Share) | 100%-150% | $0 | $700 | 20% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 1 (2017) (87% AV Cost Share) | 150%-200% | $450 | $2,250 | 20% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 1 (2017) (73% AV Cost Share) | 200%-250% | $3,500 | $5,450 | 20% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 1 (2017) (Limited Cost Share) | 300% and Above, AIAN* | $5,500 | $6,500 | 20% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 1 (2017) (Zero Cost Share) | 300% and Below, AIAN* | $0 | $0 | 0% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 1 (2017) (Standard Cost Share) | 250% and Above | $5,500 | $6,500 | 20% Coinsurance | View PDF | View PDF |
| Ambetter Balanced Care 1 (2017) (Standard Cost Share) | 250% and Above | $5,500 | $6,500 | 20% Coinsurance | View PDF | View PDF |
| Ambetter Secure Care 1 (2017) with 3 Free PCP Visits (Standard Cost Share) | 250% and Above | $1,000 | $6,350 | 20% Coinsurance | View PDF | View PDF |
| Ambetter Secure Care 1 (2017) with 3 Free PCP Visits (Standard Cost Share) | 250% and Above | $1,000 | $6,350 | 20% Coinsurance | View PDF | View PDF |
| Ambetter Secure Care 1 (2017) with 3 Free PCP Visits (Zero Cost Share) | 300% and Below, AIAN* | $0 | $0 | 0% Coinsurance | View PDF | View PDF |
| Ambetter Secure Care 1 (2017) with 3 Free PCP Visits (Limited Cost Share) | 300% and Above, AIAN* | $1,000 | $6,350 | 20% Coinsurance | View PDF | View PDF |
| *AIAN is an abbreviation for American Indian/Alaskan Native, and certain plans are available specifically for American Indians and Alaskan Natives. |
Cleveland Hospital Network
Kindred Hospital- Cleveland Gateway |
Kindred Hospital – Cleveland Gateway 2351 E 22nd Street 7th Floor |
(216) 592-2830 |
||||
St Vincent Charity Medical Center |
St. Vincent Charity Hospital St Vincent Charity Medical Center 2351 E 22nd Street |
(216) 363-7402 |
||||
Grace Hospital |
Grace Hospital 2307 W 14th Street |
(216) 687-1500 |
||||
Lutheran Hospital |
Lutheran Hospital Lutheran Hospital 1730 W 25th Street |
(216) 696-4300 |
||||
The Metrohealth System |
The Metrohealth Systems The Metrohealth System … 2500 Metrohealth Drive |
(216) 778-4758 |
||||
Cleveland Clinic Children’s Hospital For Rehab |
Cleveland Clinic Childrens Hospital For Rehab 2801 Martin Luther King Jr Drive |
(216) 430-8075 |
||||
UH Cleveland Medical Center |
Rainbow Babies Childrens UH Cleveland Medical Center 11100 Euclid Avenue |
(216) 844-1000 |
||||
UH Cleveland Medical Center |
University Hospitals of Cleveland UH Cleveland Medical Center 11100 Euclid Avenue |
(216) 844-7674 |
||||
Kindred Hospital- Cleveland |
Kindred Hospital-Cleveland Kindred Hospital-Cleveland 11900 Fairhill Road |
(216) 983-8030 |
||||
Marymount Hospital |
Marymount Hospital Marymount Hospital 12300 McCracken Road |
(216) 587-8108 |
||||
Lakewood Hospital |
Lakewood Hospital Lakewood Hospital 14519 Detroit Avenue |
(216) 521-4200 |
||||
Meridia South Pointe Hospital |
South Pointe Hospital Meridia South Pointe Hospital 4110 Warrensville Center Road |
(216) 636-8114 |
||||
University Hospitals Parma Medical Center |
Parma Community General Hospital University Hospitals Parma Medical Center 7007 Powers Boulevard |
(440) 743-4242 |
||||
Fairview Hospital |
Fairview Hospital Fairview Hospital 18101 Lorain Avenue |
(216) 476-7000 |
||||
University Hospitals Rehabilitation Hospital |
University Hospitals Rehabilitation Hospital University Hospitals Rehabilitation Hospital 23333 Harvard Road |
(216) 593-2200 |
||||
UH Ahuja Medical Center |
University Hospitals Ahuja Medical Center UH Ahuja Medical Center 3999 Richmond Road |
(216) 593-5887 |
||||
UH Regional Hospitals |
UHHS – Bedford Medical Center UH Regional Hospitals 44 Blaine Avenue |
(216) 439-2000 |
||||
Euclid Hospital- Rehabilitation Unit |
EUCLID HOSPITAL Euclid Hospital-Rehabilitation Unit 18901 Lake Shore Boulevard |
(216) 531-9000 |
||||
Meridia Euclid Hospital |
Euclid Hospital Meridia Euclid Hospital 18901 Lake Shore Boulevard |
(216) 636-8114 |
||||
Southwest General Hospital |
Southwest General Health Center 18697 Bagley Road |
(440) 816-8404 |
||||
Ambetter 2017 Drug Formulary
Contact Us
Phone: (312) 726-6565
Email: [email protected]